This diagram was given to me by a new sleep patient once. It was given to them by their prior sleep specialist at their new visit with them. Many years later, they were still suffering from poor sleep and excessive daytime sleepiness from what turned out to be a relatively straight forward cause. We were able to address it without even needing a new sleep study, just a long conversation discussing their sleep issues. Anyway, I asked them if I could make a copy because it made me laugh. How intimidating is this chart?! Why would I show someone this? It looks like the slide from some scientific meeting.
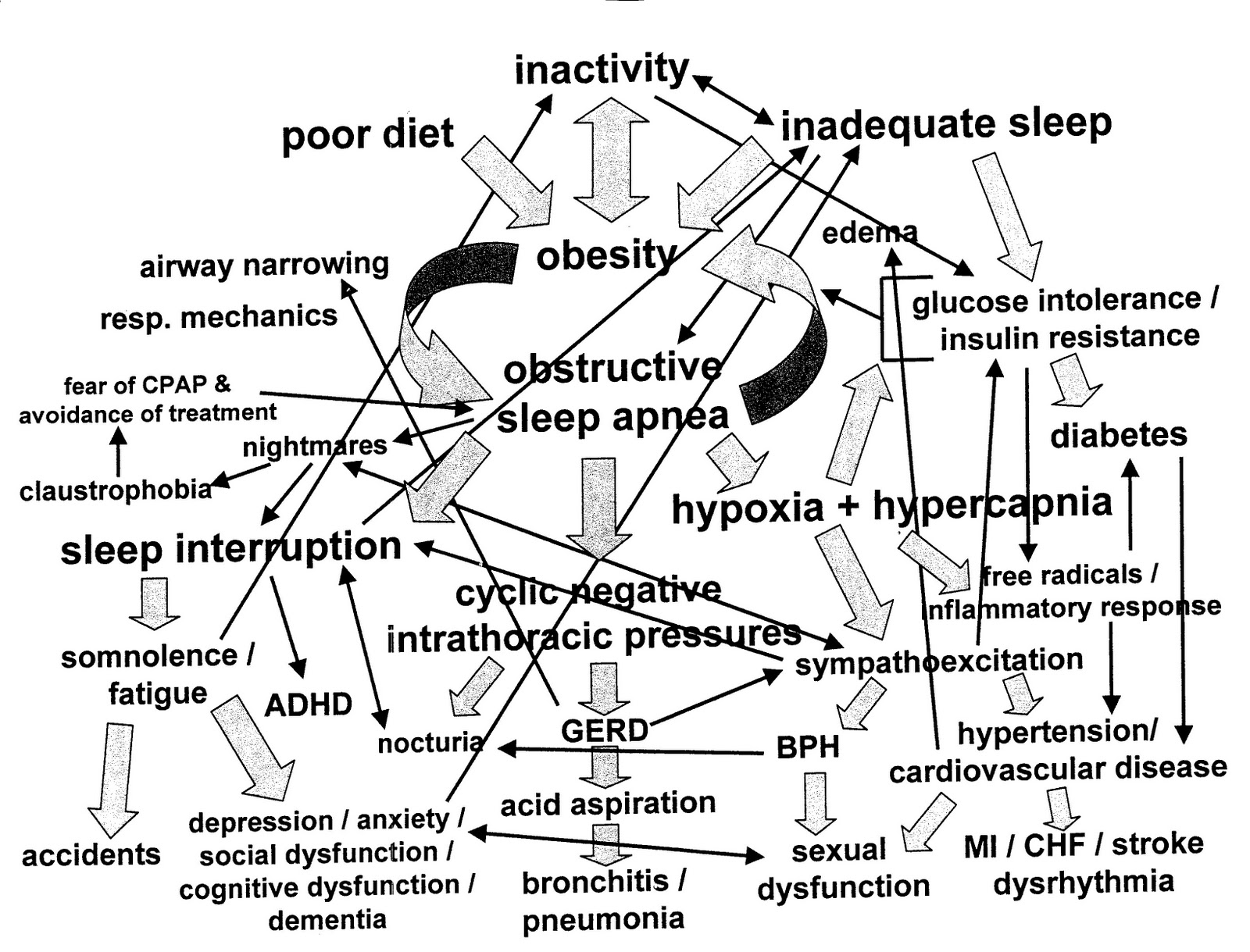
I decided that if you could understand that diagram, you could probably work this and then procede to fly off in it after I showed you the above diagram:

The reality is that yes, Sleep Medicine can be very complex. It is at the intersection of many medical disciplines: Neurology, Pulmonology, Cardiology, Otolaryngology, Psychiatry, and the implications of different sleep disorders (More than 85 different sleep disorders last count) cross-affects many different medical specialties.
But, many of these sleep disorders can be evaluated and diagnosed without requiring an overnight sleep study.
If you do need a sleep study, we essentially look at the following basic parameters:

-Sleep stages (notice the stage REM dreaming in black)
-Body position (This person started on their right, then went to their back, then left... never on their stomach)
-Oxygenation (We want it to stay close to 100%. This person dropped severely)
-Respiratory events (There are many types of respiratory events. This person had mainly two types but many of them)
-CPAP (You can see it starts in the latter part of the night, and we increase the pressure to try and find one that stops or markedly improves the number of respiratory events. This person had a trend of improvement but may need more work)
-Arousals (This is arousals from all different types of things: breathing issues, leg movements, pain, bed partner snoring... although we have to figure some of this out more by discussion than this estimate alone. This at least tells us a basic idea of what all woke you up this particular night)
-Periodic Limb (leg) Movements during your sleep (not a problem for this individual)
We can check many other things as well, such as carbon monoxide levels, or we can add a full EEG to your head to look not only for sleep stages with our basic EEG, but for actual nocturnal seizures. We also do other tests for things such as Narcolepsy or for more complex sleep apnea or assessment of daytime wakefulness.
But in your average initial diagnostic polysomnogram (PSG), the fancy word for sleep study, these are the basic things we look at and utilize to help determine how an average night of sleep unfolds for you.
So I hope when you go to discuss these things with your sleep specialist physician, you can just relax and tell him or her what is going on, and let them figure out where to fly from there.