There is no test for Essential Tremor, although tests can rule out other causes. This is a clinical diagnosis, based on history and exam.
Essential tremor arises most often in the hands, but can be present in the legs or head/neck as well. It can also affect the voice as well but this is uncommon.
When it starts on one side, it usually involves the other side to some degree within 3, sometimes 5 years.
It can occur at any age but is usually more common in adults (middle aged and above).
It is NOT caused by anything, medication nor disease. It is most often confused with the tremor of Parkinson's. Although these tremors can look similar sometimes, they are different and have a different cause.
Essential tremor is often inherited, present to some degree in a parent or grandparent, but many factors may cloud this element of the family history such as an early death from some other cause before the tremor expressed itself to a clinical degree. This means that there is a gene that causes essential tremor (called familial tremor at this point) in most cases, but in those without such a familial history, the exact cause is unknown.
Essential tremor is often progressive, but often slowly. It is rare for it to NOT progress over time to some degree, but ALSO RARE to progress rapidly OR to a severe degree.
If it is isolated to the head/neck then it usually is noticed by others before it is noticed by the patient themselves. They usually seek treatment only because it is concerning to them that other people keep noticing, or they are annoyed that everyone thinks they have Parkinson's disease. Essential tremor, when progressing in the hands, becomes problematic because it starts to interfere with handwriting, filling out paperwork for work and bills, typing, tying shoes
Essential tremor is worsened by: stressful situations, caffeine, a hot summer day/cold winter day, fatigue, missed meals/low blood sugar.
Now, I do think some differences between Essential Tremor and a Parkinsonian Tremor should be addressed here, to both characterize the tremor further, and differentiate from the fear most people have: that it represents the beginning of the constellation of symptoms associated with Parkinson's Disease.
Essential Tremor:
High frequency (fast 4-6 per second) In other words, the tremor moves back and forth quickly.
Worse with movements like holding a glass of water outstretched (action or kinetic tremor)
Usually NOT associated with gait problems.... when it IS, it is usually because of ataxia (dysfunction of coordination) rather than the issues with the neurotransmitter dopamine which causes a different gait problem in Parkinson's.
Can be in the head, voice, as well as the hands and legs. It can be in one hand or the other, and is often worse on one side.
Parkinsonian Tremor:
Lower frequency (3-5 per second) The shake is slower.
It is more noticeable at rest (rest tremor), NOT movement. In fact it often resolves or lessens when the hand is being used.
Often associated with stooped posture/shuffling gait, or other motor symptoms which are NOT seen with essential tremor.
Is usually in the hands or legs first, usually NOT the voice, and only late is it seen in the head. Like essential tremor, it can be present or worse on one side only.
Another difference: Response to alcohol.
Now I definitely do NOT recommend drinking alcohol to treat essential tremor. In fact, there are patients who develop problems with alcohol because essential tremor almost always improves with alcohol. I had one of my patients do this little diagnostic experiment at home because, despite my reassurances that they had Essential Tremor, they seemed a little concerned about having Parkinson's when it came time to end our visit.
The test below is the suspended spiral drawing test. You put a piece of paper on your lap, take a pen in your hand, suspend it in the air without resting your arm/elbow on anything and draw a steady spiral from in to out. The normal spiral is a smooth thing and a jagged spiral is the expression of the action tremor classic for Essential Tremor. Now, for some reason, alcohol blunts the tremor for a short time. It's a cheap test for those in which there is no contraindication to trying it.
Day 1 Trial with Wine
(In the evening, before and then 30 minutes after wine)
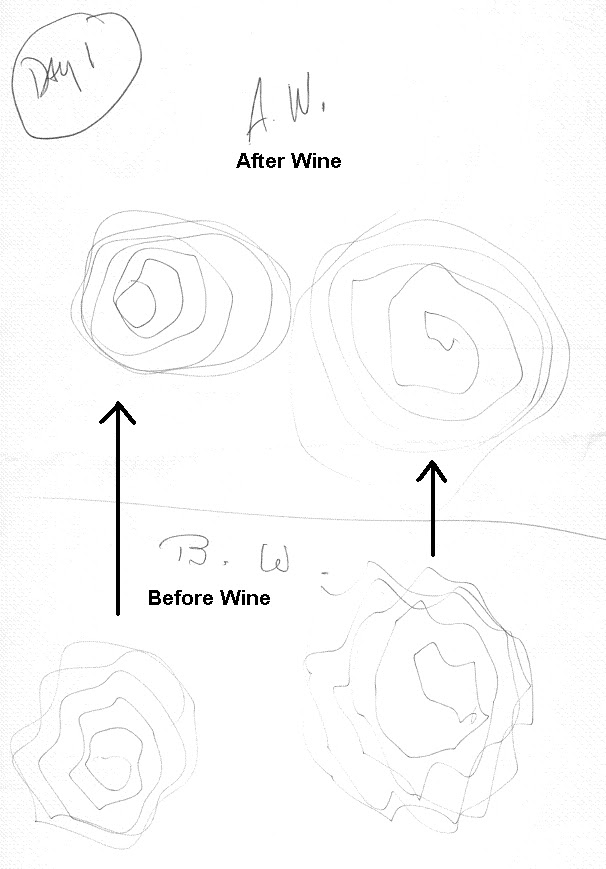
Trial 2
(I think the patient was having quite a bit of fun with the testing)

Long-term treatment for essential tremor involves two main medications which have strong evidence in the literature behind their effectiveness (Since alcohol is only helpful for a short period and in the long-term causes more problems than Essential Tremor, AND can cause a tremor itself). There is no cure for essential tremor.
The first to try is long acting Propranolol. Once I hit more than 240mg a day in divided dose, it's time to consider Primidone. This one is more likely to have side effects, but the dose needed is sometime much higher (up to 200mg per day). If these don't work, sometimes a lower dose of each together will work.
The next in line, Sotalol and Atenolol which are cousins of Propranolol, Gabapentin, Topiramate, Alprazolam, Methazolamide, and Clozapine have less robust data behind their effectiveness, and they can have their untoward side effects as well, but can be tried.
For some people, the tremor is very stubborn to treatment and really inhibits lifestyle. In these rare individuals, Botulinum toxin A ("Botox") can be injected into the muscles to force them to relax, even though some mild side effect weakness usually comes with this treatment.
Now, very VERY few individuals need further treatment considerations. But if you're reading this, you should know that they are out there.They include surgical interventions that affect the part of the brain, the basal ganglia, that has an important role in coordinating our motor movements to suppress a tremor. By surgically intervening in various parts of this complex piece of neuroanatomic "on" and "off" switches, the tremor can be improved.
Deep brain stimulation (DBS): An electrode is surgically placed into the thalamus of the basal ganglia and attached to a pacemaker under the skin near the collarbone. The pacemaker sense pulses of electricity to the thalamus to inhibit the tremors. It is really only used for bad limb tremors, not head or voice tremors. There are currently very few places that do this procedure.
Thalamotomy: An actual lesion is surgically made in the thalamus (one side only).
Gamma knife surgery: It is essentially a thalamotomy, like above, but done without actual cutting, but rather, but focusing radiation externally to cause the lesion deep in the brain at this location. This is the newest invasive treatment at the time of this writing and is still being evaluated.